Tongue Cancer
The Center for Disease Control and Prevention (CDC) estimates more than 30,000 new cases of oral and pharyngeal cancer are diagnosed each year . One of the most commonly affected sites of oral cancer is the lateral border of the tongue and squamous cell carcinoma makes up the majority of lesions found here. The 5-year survival rate for oral cancer is approximately 50% and treatment of this disease with surgery has become one of the most important treatment modality for these patients. The preferred method of surgery is glossectomy, which is removal of the tongue tumor in addition to an extra margin of healthy tissue. Resected area may be closed primarily with sutures or with a free flap usually from the radial forearm. Size of the tumor and the extent of surgery often affect the patients’ tongue motor adaptation. Cancer patients used in this research had smaller tumor of the lateral tongue, T1 or T2 that were closed primarily with suture (see Figure 1). T refers to the size of the tumor using the TNM system (National Cancer Institute). In the tongue, T1 is <2cm in the largest dimension and T2 is 2-4cm in the largest dimension. All these patients were also N0 and M0 (nolymph node involvement or metastasis).
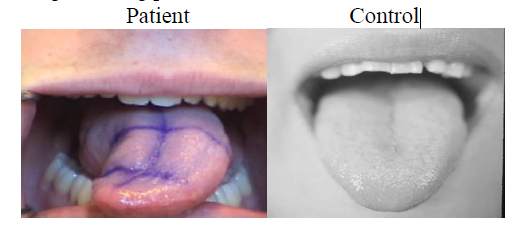
Figure 1. Control tongue during protrusion does not deviate
MRI : Magnetic Resonance Imaging
Since the inception of Magnetic Resonance Imaging (MRI), many studies have been done on soft tissue analysis. Using a powerful magnetic field, sensors detect radio frequency signals emitted from excited hydrogen atoms, such as from water molecules. As our tissues are filled with water molecules, MRI provides researchers with great visibility of soft tissue in our body while hard tissue such as bone will show as radiolucent. High resolution MRI is able to show tissue shapes and structures with great details. In this experiment, we also employed cine-MRI (like cinema) where series of MRI are linked together to form a movie of soft tissue in motion. Cine-MRI is of particular importance in this research as we are able to track the changes during production of phonemes. Unlike high-resolution MRI, cine-MRI is of lower quality (pixel resolution) and one cannot differentiate fine details. However, the purpose of this study was not to delineate one muscle from another. Instead, we wanted to observe the entire tongue volume shifts in the tongue tissue between /uh/ and /s/, thus cine-MRI was the ideal imaging modality to observe and measure these changes.
Palate Features and /s/ types
During the production of /s/ in “a souk”, Stone et al [2013] identified that the tongue tip may be up or down (See Figure 2). They classified this as apical or laminal /s/ respectively. Stone et al [2013] proposed and noticed that the palate height affected the type of /s/ produced during “a souk”. In that study, control subjects (unaffected tongue) with high palate displayed more laminal /s/ and low palate showed apical /s/. However in glossectomy patients, palate height did not seem to affect /s/ type and instead favored laminal /s/. This may be related to the difficulty in patients controlling the tip of the tongue due to the resection. Although tip of the tongue is preserved during surgery, discontinuous fibers and reduced motor innervation of the tongue makes control of the tongue challenging. Thus differences in anteriority of /s/ types are expected to be seen during /uh/ to /s/. This study also hopes to investigate the differences in anteriority of high vs. low palate subjects as palate height appeared to influence the type of /s/ made during “a souk”.

Figure 2. Apical vs. Laminal tongue shape at /s/.
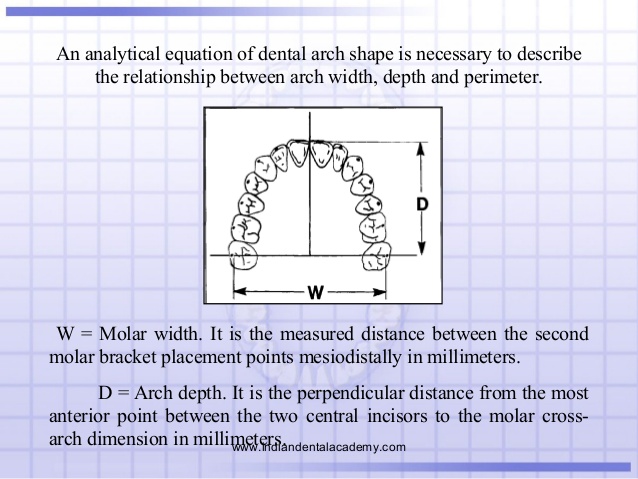
Arch Perimeter and Canine Width
In addition to palate height, other features of the oral cavity may influence tongue anteriority. Most notably the teeth surrounding the tongue have the potential to influence tongue anteriority as the teeth create a physical barrier for the tongue both laterally and anterior. In this study, only the upper arch was taken into consideration as most of the contact with the tongue was made with the upper arch and not with the lower arch during “a souk”. Arch perimeter is defined as the distance formed along the cusp tip of dis tobuccal 1st maxillary molar (M1) to the contra-lateral disto-buccal cusp tip 1st maxillary molar (See Figure 3). Arch perimeter is important in anteriority because the teeth form the physical boundaries of the oral cavity thus limiting the movement of the tongue anteriorly. This experiment also measured upper canine width from cusp tip to cusp tip. As canines are the anchoring teeth and one of the first teeth to come in contact with the tongue during speech, canine width may influence anteriority during speech.
Figure 3. Arch perimeter is shown on this cast labeled in red. Canine width is labeled in
blue.