Stereotactic radiosurgery
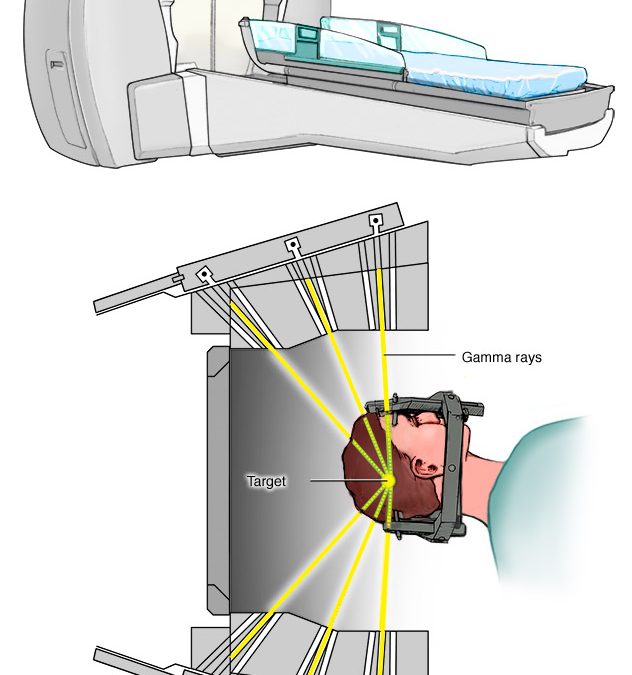
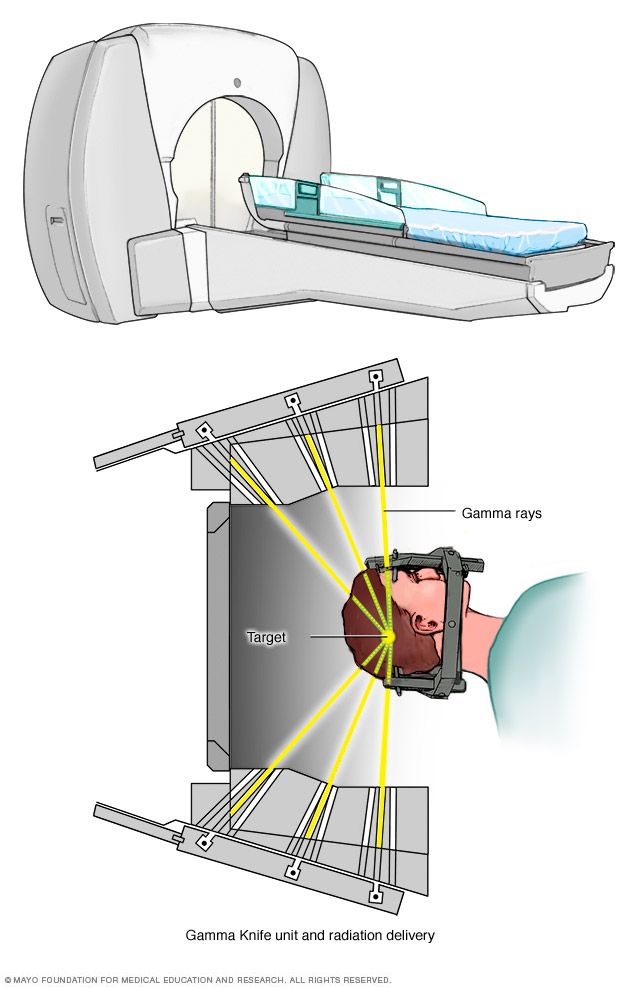
Stereotactic radiosurgery (SRS) is a non-invasive alternative to surgery for various types of head and neck disease, including cancer. As opposed to stereotactic radiotherapy, in which smaller doses of radiation are given over a large number of treatment sessions, SRS is a radiation therapy treatment system in which radiation is delivered to the patient in a single treatment session, called a fraction. In SRS, beams of radiation are applied to a target, denoted as the gross tumor volume (GTV), to achieve a specic prescribed dose while minimizing harm to nearby organs at risk (OARs).
In this thesis, we will study radiosurgery done using the Leskell Gamma Knife R (LGK) PerfexionTM (PFX, Elekta, Stockholm, Sweden) device. LGK PFX is an SRS
device that can accurately deliver high-dose radiation to target structures within a patient. To accomplish this task, the PFX simultaneously produces beams of radiation from eight sectors of radiation sources surrounding the patient. A single collimator array determines the size of each of the beams of radiation, and each sector’s beam can be driven independently to a diameter of 4mm, 8mm or 16mm, or deliver no radiation at all. During a treatment plan, the patient is secured to a mechanical couch, and this couch is positioned so that the sectors are aimed at a precise location, called an isocenter, for a planned duration of time. A combination of isocenter location, duration, and collimator size is called a shot.
Older LGK devices required manual intervention between shots, meaning that complex treatment plans were impractical. As a result, studies on LGK SRS optimization done using previous models of the LGK assume a small, xed number of isocenters and focus mostly on the optimization problem of deciding on isocenter locations and durations within a target. More recent research in LGK SRS optimization uses a two-stage approach : First, determine good isocenter locations using geometrybased heuristics; then, run a sector duration optimization to nd the treatment time of all of the radiation beams to apply appropriate dose to the GTV. In the rst stage, when trying to place isocenters, the quantity and location of shots are chosen heuristically based on the geometry of the target rather than on dosimetric calculations; popular heuristic algorithms incorporate different heuristics such as grassre, skeletonization, sphere-covering, sphere-packing, and genetic algorithms. In the second stage, isocenters are assumed to be xed, and the resulting problem to nd the durations of each radiation beam can be solved. This problem is often cast as a convex optimization problem or, more simply, as a linear program. We have not found any work showing how close the geometry-based approaches come to nding optimal isocenter locations; however, these geometric approaches often yield good practical results.
Isocenter selection and sector duration can be combined into a single exact problem formulation called the sector duration and isocenter optimization problem (SDIO). SDIO combines the isocenter location stage and the sector duration optimization stage into a single mixed integer optimization problem. This approach was previously demonstrated to nd acceptable treatment plans; however, the technique used to solve the one-stage MILP formulation required some restrictions on the solution space in the form of tight upper and lower bounds on the number of isocenters chosen, and heavy approx imations in terms of reductions to the number of constraints and decision variables in a process called sampling, to achieve tractability.
Stereotactic radiosurgery
