Bone reconstruction options for the Mandible
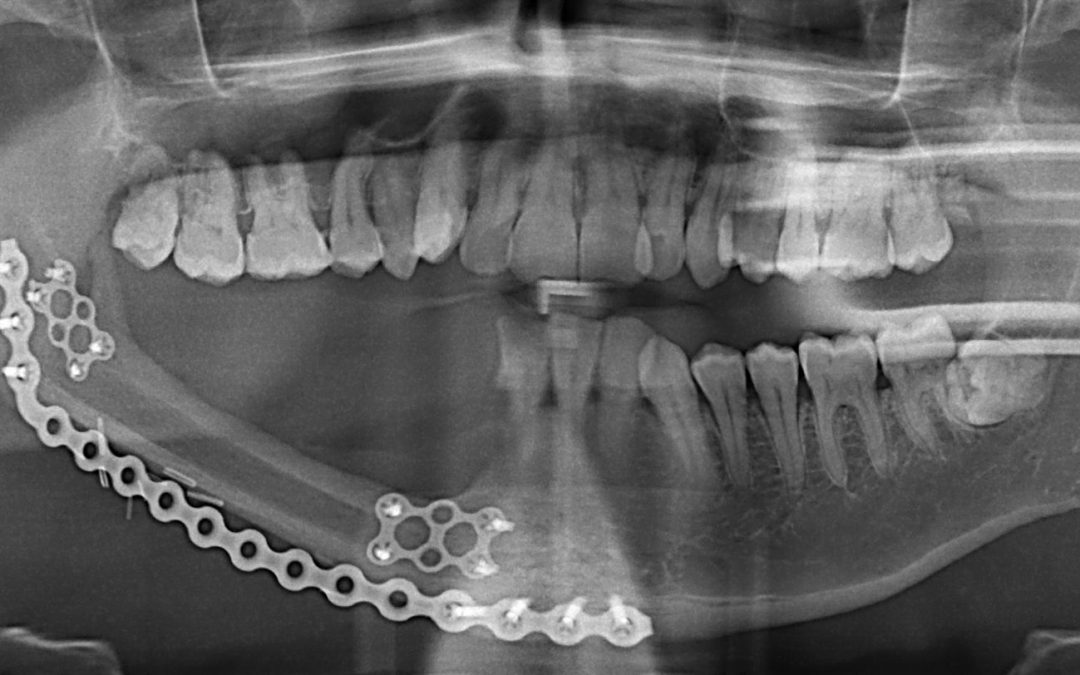
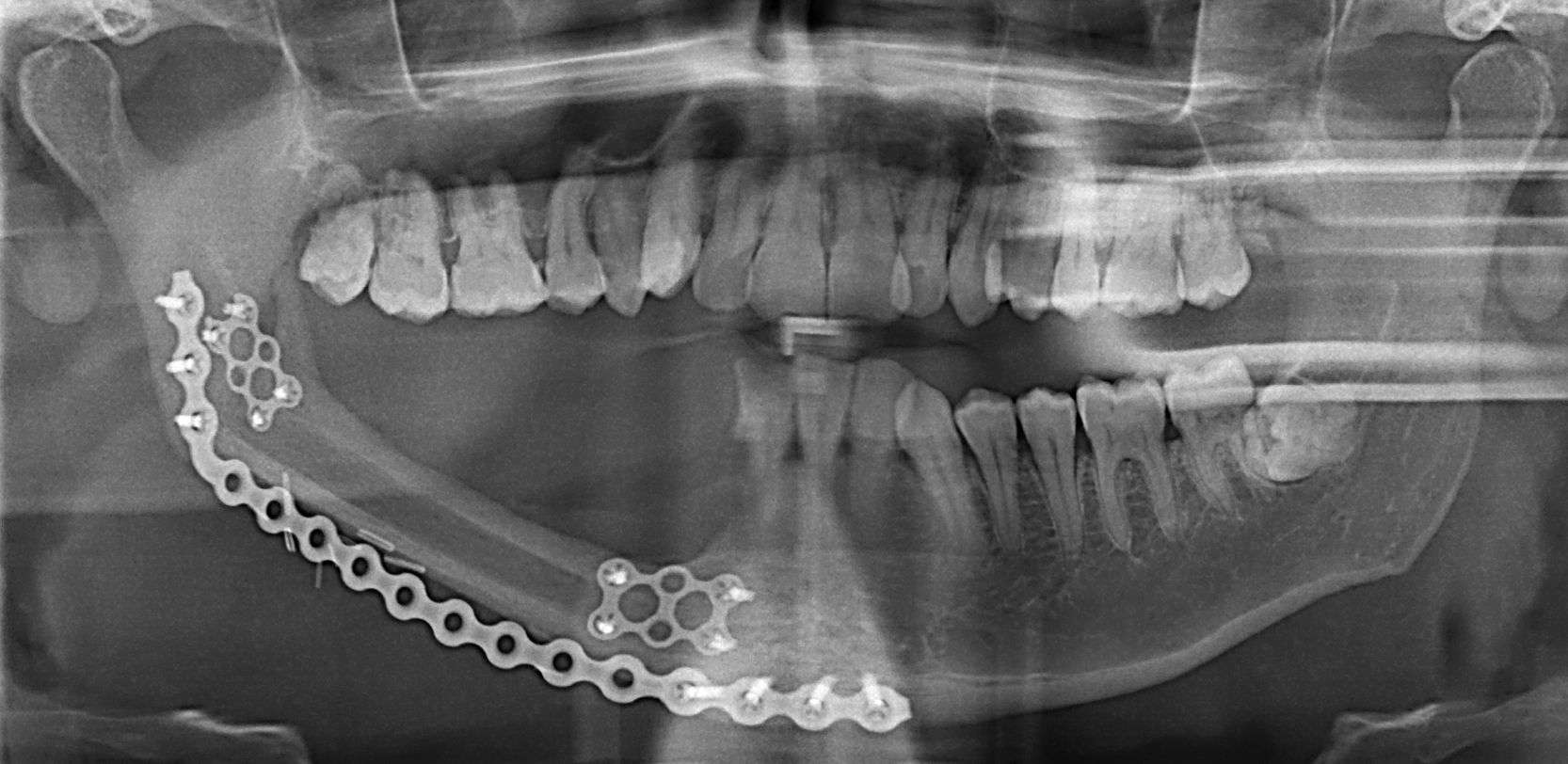
Reconstruction of the lower jaw avoids severe functional and esthetic debilitation. The ideal reconstruction should re-establish oral continuity, allow for dental rehabilitation, restore sensation of the lower lip, restore facial form and cosmesis, and must withstand radiation therapy if needed. The continuity of the mandible can be maintained with titanium reconstruction plates and screws alone. This is usually preserved for patients who are poor surgical candidates, small lateral defects, and patients with short life expectancy. However, bony reconstruction is needed to avoid the likely hardware failure especially in larger defects. It provides better esthetics and allow for dental rehabilitation with dental implants or prosthesis. Some of these defects may have a soft tissue component (e.g. malignant tumors and gun shot wounds), which also need to be addressed prior to the bony reconstruction or simultaneously. Two general categories of reconstruction techniques are available for defects of the Mandible. Non-vascularized cortico-cancellous is the older technique that is still used today for small defects (less than 5 cm) without history of radiation or concomitant soft tissue defect. It has the advantages of higher bone volume, shorter surgical procedure, easier technique, and less morbidity. The most common donor site is the anterior iliac bone, which can provide about 50 CC of cortico-cancellous bone.15,16 A posterior approach is used to harvest bone from the iliac bone and is reported to provide about twice the amount of the anterior iliac approach with less morbidity However, it requires switching to a prone position intra-operatively excluding simultaneous head and hip approach (two teams) and risking extubation. Costochondral rib grafts have proved useful for the reconstruction of Mandibular defect involving the temporomandibular joint (TMJ), especially in growing patients. Other sources include the calvarium, the tibia, Mandibular chin, and ramus. More recently, vascularized bone graft has become the standard for the reconstruction of large Mandibular defects, those with soft tissue defect or after radiation
to the area. It has a high success rate and provides reconstruction in one stage. Potential vascularized bony flaps include the fibula, ileum, scapula, and radius bones. The workhorse for mandibular reconstruction is the vascularized fibula free flap (FFF). It was introduced in 1975 by Taylor et al for the treatment of post traumatic defect of the lower extremity. In 1989, Hidalgo was the first to describe its use to reconstruct the Mandible. This flap is based on the peroneal vessels (artery and 2 vena comitantes) that are one of the main three branches supplying the lower extremity and the foot, along with anterior and posterior tibial vessels. It can provide up to 27 cm of bone and allow segmentation without devascularization. It allows two-team approach, thus reducing the operative time. Moreover, It can provide composite soft tissue and bone reconstruction based on skin perforators. However, it has relatively small bone thickness compared to the Mandible. Different imaging modalities are used preoperatively to assess the patency of the blood vessels of the lower extremity and to rule out anatomic variations that would exclude the use of the FFF. Angiography is the gold standard but due to its invasive nature and low incidence of anatomic variation, less invasive techniques are routinely used. Those include computed tomography angiogram (CTA), magnetic resonance angiogram (MRA), and color-flow Doppler. Reconstruction of shorter segments of the Mandible can be achieved using a single segment of the fibula, creating proximal and distal bony gaps between the fibula and the Mandible. However, if the continuity defect is long it will require the segmentation of the fibula to imitate the curvatures of the Mandible by removing a wedge of the fibula bone. This will result in the creation of a third and possibly a fourth bony gaps between the segments of fibula. Fibular segments are secured in place using titanium plates and screws.
Bone reconstruction options for the Mandible
