Anatomy and physiology of the Mandible
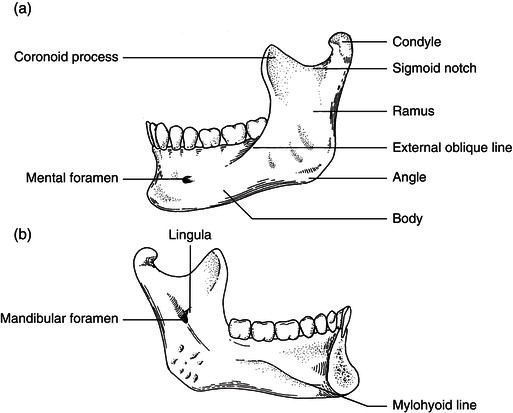
The lower jaw (mandible) consists of a horseshoe-shaped segment harboring the alveolar segment that supports the dentition. It connects posteriorly with two vertical rami, which articulate with the temporal bones via round condylar heads forming the temporomandibular joints (TMJs). It defines the appearance and profile of the lower third of the face. The Mandible serves as the site of attachment of several muscles and ligaments including the muscles of mastication and the suprahyoid muscle groups. The muscles of mastication include the masseter, medial pterygoid, lateral pterygoid, and temporalis muscles. Their actions result in Mandibular opening, closing, and lateral excursions. The Mandible is exposed to significant amount of forces and stress during speech, yawning and mastication. Tensile forces mainly affect the superior part of the Mandible while compressive forces affect the inferior part. Champy et al defined the lines, just below the roots of the teeth, where tensile and compressive forces are equal.9 Anterior to the canines (Symphysis area) the Mandible is affected by a torque of alternating tension and compression zones. The Mandible is thicker anteriorly in the symphysis area with an average thickness of 14 mm in males and 13.2 mm in females.10 Classification of Mandibular continuity defects Continuity defects of the Mandible may result from trauma or surgical treatment. Several diseases require surgical resection of the affected segment of the Mandible. These include benign and malignant tumors, resistant bone marrow infection (osteomyelitis), and bone necrosis secondary to radiation or bisphosphonate medication. Several classifications exist to characterize the continuity defect. Jewer et al proposed a classification system where the area between the lower canines is designated “C” for central segment. Lateral defects not involving the condyle is designated “L” while hemimandibular defects involving the condyle are designated “H”. Boyd et al added to this classification the soft tissue component using lower case letters; skin (s), mucosa (m), or osseous only (o). A more complex classification was described by David et el into six classes depending on location, size and laterality of the defect. More recently, Baumann et al suggested a simple and useful classification system derived from their experience in the reconstruction of osteoradionecrosis Mandibular defects. A type one defect is a segmental defect where the condyle is intact while a type two defect is posterior or hemimandibular defect where the condyle is missing. They further classified the defect based on the soft tissue involvement into (a) simple mucosal defect and (b) through and through soft tissue defect.
Anatomy and physiology of the Mandible
